While revascularization clearly decreases symptoms and increases walking distance, the decision of whether to proceed with revascularization is complex. Ideally, the individual patient’s clinical features, anatomic characteristics, and personal preferences all must be assessed and integrated by both the patient and provider to facilitate a shared decision-making strategy.
Lesion-based considerations: Arterial duplex ultrasonography, CTA, and MRA offer an understanding of the patient’s anatomy and help guide the decision to revascularize and the method of revascularization. Certain lesion subsets are uniquely amenable to revascularization due to predictable technical success rates and durability. Lesion characteristics that favor endovascular therapy include the following: short segments, minimal calcification, absence of total occlusions, and the presence of greater than single vessel infrapopliteal vessel runoff. Conversely, certain lesion subsets present technical challenges and less favorable durability at follow-up, such as long lesion length, total occlusion, heavy calcification, and impaired infrapopliteal runoff. Such lesions should prompt consideration for bypass surgery if an autologous vein is present and the patient’s clinical status allows for it.
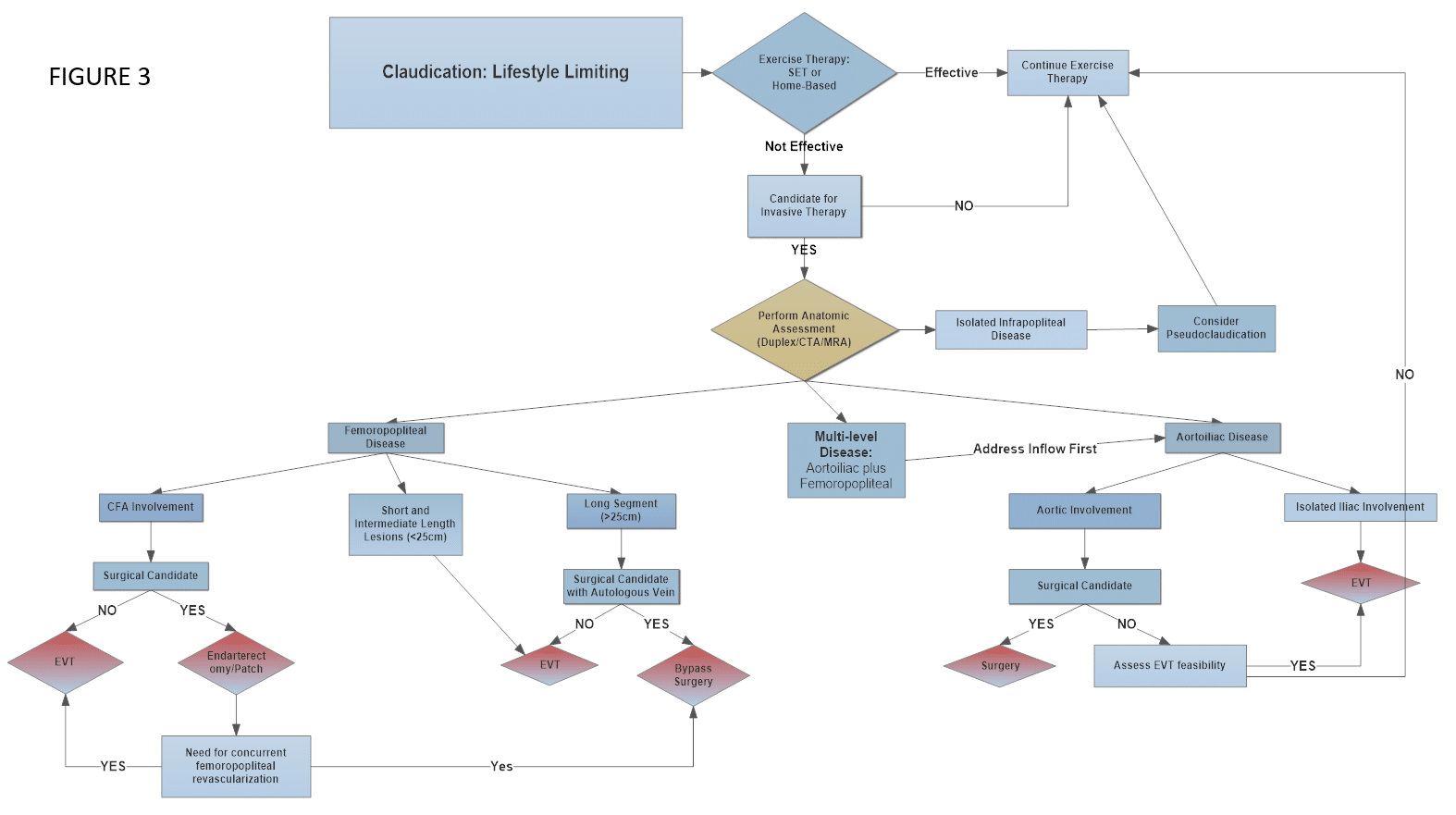
Figure 3 depicts one possible algorithm for the management lifestyle-limiting claudication. The algorithm provides a loose framework to help guide decision-making. Ultimately, the revascularization strategy should be individualized to each patient based on clinical features, anatomic make-up, and personal wishes. A few guiding principles are worth specific mention.
- Inflow first: Stenoses/occlusions of the aorta, iliac arteries, and common femoral arteries should be revascularized before more distal femoropopliteal disease. Inflow interventions are characterized by good technical success and excellent long-term patency. Most importantly, an inflow intervention often sufficiently relieves claudication, thus obviating more distal intervention.
- Shorter lesions do better: Restenosis and repeated interventions occur earlier and more frequently in longer segment stenoses and occlusions. As such, surgical bypass should be considered if an autologous vein is present.
- Comorbid conditions often affect revascularization decisions: Concomitant coronary artery disease, cardiomyopathy, cerebrovascular disease, and advanced age are common findings in patients with claudication. As such, the revascularization strategy must be formulated with operative/procedural risk in mind.
- Patient input: When noninvasive, surgical, and percutaneous options are all being considered, patient input becomes very relevant. True patient understanding about the risks of revascularization (surgery or percutaneous), the likelihood of technical success, and the rates of restenosis is important.
- Available skill: The skills of the treating provider may impact the revascularization modality. This is acceptable in many such cases, as there is still a great deal of subjectivity in the management of this patient population. The provider’s skills, experience, and comfort level with a particular treatment modality may improve outcomes in the specific patient’s treatment environment.
(Click image to enlarge)